
Part II covered clinical
reasoning, postural deviations, and clinical context while Part I
covered posture, evidence and clinical context. As we reach the end of
this posture-related journey, I wanted to touch on a few different clinical key
points. Not to fully dive in, but to bring light to areas of clinical practice
and posture that might inspire reflection. So to begin let’s resume the conversation
from the last post- When does a postural deviation matter? How do we sieve out
the clinically important details when sometimes our patients come in with SO
many deviations from the norm?
As my clinical fellowship
mentor Tim McMahon, pointed out to me during one of our fellowship mentoring
sessions, it is extremely to want to see everything outside the norm as a
problem, getting lost in the weeds and missing the veritable “smoking gun”. So
then, it is best to prioritize the most obvious findings and use clinical
reasoning to whittle down the red herrings.
As explained by the portion
of clinical reasoning that includes the “reflective process of inquiry
and analysis carried out by a health professional in collaboration with
the patient” 1. Careful selection of components of the movement and
physical exam must be based on reflection of patient context and the verbal and
physical subjective. In other words, does that deviation contribute to
the patient’s clinical presentation or is it a natural and non-problematic
adaptation?
A hypothetical example being
that scapular mal-positioning or scapular dyskinesia is not always a problem.
What if the dyskinesia is a functional adaptation with an appropriate movement buffer
zone capacity (adequate thoracic spine, sternoclavicular, acromioclavicular,
scapulothoracic, and glenohumeral mobility)? But then again, people who have
functionally adapted with appropriate buffer zones usually are not entering the
clinic unless they are looking for preventative treatment/measures (of which we
should be equally prepared for).
SO for the majority of patients who DO have pain and present with scapular mal-positioning or dyskinesia, we have to test and inquire if the scapular positioning is a contributing factor to their pain by proxy of (and not limited to) a neuromuscular timing issue or a need for increased movement buffer zones.
SO for the majority of patients who DO have pain and present with scapular mal-positioning or dyskinesia, we have to test and inquire if the scapular positioning is a contributing factor to their pain by proxy of (and not limited to) a neuromuscular timing issue or a need for increased movement buffer zones.
So putting it into context- I
had a patient who had glaringly obvious upper crossed syndrome posturing
(forward head, rounded shoulders as described by Janda) and forward drawn
positioning (as described by the Prague School of Rehabilitation) with ongoing
jaw pain and headaches. This person had seen 5 other therapists who had treated
and gave her all sorts of exercises addressing their upper quarter to some
relief but no lasting results. They were about to give up and were only in the
office because insurance was needing “failed rehab” for surgical procedures
coverage. The “smoking gun” was noted
when they mentioned in passing that their pain primarily came on when standing
or walking. When watching their posture, looking at the “stacking” of body
parts, you could tell that most of their posture was being driven in standing
and walking from limited dorsiflexion, particularly the ipsilateral
ankle of the painful side. Assessment concluded passive and active dorsiflexion
deficits along with an active soleus myofascial trigger point that had referral
to their jaw (yes, the soleus can refer to the jaw. It is rare, but it is a
known occurrence and shows the importance of understanding myofascial pain!) 1.
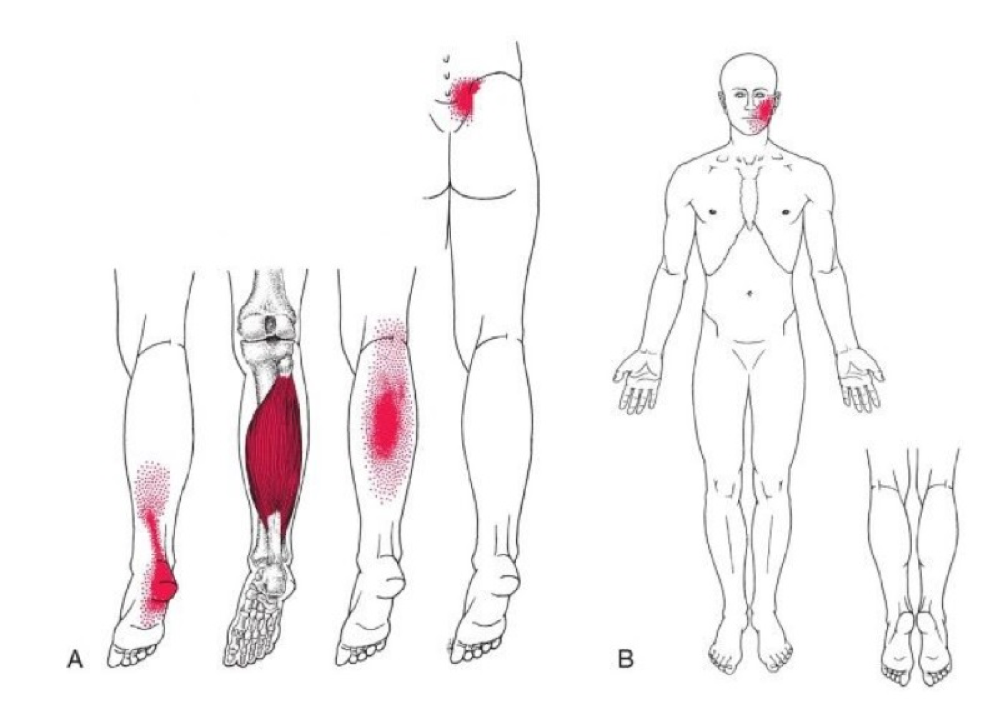
(Figure 66 in Geist K, Donnelly D. Chapter 66 Soleus and Plantaris Muscles “Joggers Heel”. In: Donnelly JM, Fernandez-de-las-Penas C, Finnegan M, Freeman J. Myofascial Pain and Dysfunction The Trigger Point Manual. Philadelphia, PA: Wolters Kluwer; 2019.)
After treating the soleus and
talocrural joint (driving the inability to dorsiflex) the patient within the
week had significantly decreased symptoms in their jaw and headaches with an
eventual resolvent of all symptoms. An uncommon case for sure, but pretty
mind-blowing right? Had I continued to ignore the patient’s words and
myopically treated the deep neck flexors, the upper quarter endurance, etc, and
didn’t listen and put the patient’s full context into play, I could have
been the final straw that drove this person into a costly surgery that they may
not have needed at all. Not all postural impairments/deviations matter, but a
thorough examination and subjective does!

My inner thoughts when I finally made the appropriate clinical conclusion
Patients come to the therapy clinic for a myriad of reasons. But primarily it is because they are no longer with homeostasis of the movement system and need help to balance that out. It is then our duty as movement systems specialists to systematically find whatever is impeding them from living their life to the fullest and, to the best of our ability, empower the patient (treatment) to regain movement homeostasis.
So what are some means of
empowering patients in regards to posture? Changes to posture have their own
different categories depending on the root cause of the problem. Even the
crafted words we use for patients sometimes hold power and weight that can
either give them the intrinsic motivation and strategies to succeed or weight
down or even reverse progress. To talk about empowering patients in regards to
posture, we have to have a brief blurb on the types of changes, language, and
motivational interviewing.
Postural corrections are
usually derived from extrinsic or intrinsic changes. Extrinsic changes are more
so changes to the environment or areas that patient positions are being held.
It is to give the individual the most effective means of resisting gravity,
restore appropriate muscle length balance, decrease inappropriate tonic muscle
activity (per Dr. Vladimir Janda) and trigger point formation (per Simons and
Donnelly), and provide the best position for comfort to escape pain-inducing
positions and sleep for healing of tissues and the nervous system. Does it mean
that the patient is to be guilted for not maintaining this position constantly?
Of course not! There is no “bad posture”. Just posture held
for too long. Even the most efficient sitting or standing posture can be
cumbersome and difficult for long periods of time! Standing desks, yoga ball
chairs, posture braces while all have good intention, they miss the best
corrective factor… moving often. Give your body that variability it
craves. Don’t bother with the really expensive chair…just get up and dance for
a couple minutes guaranteed much cheaper and much more fun.
Intrinsic changes come from
increasing the buffer zones on patients. Whether it is strength or conditioning
(functional range conditioning, Kinstretch), Dynamic Neuromuscular
Stabilization (DNS) and joint centration, manual therapy to decrease pain,
whatever clinical tool you might have in your arsenal, the intent is to provide
an internal environment that will allow for restoration of the patient’s
homeostasis. Both extrinsic and intrinsic changes, however, require appropriate
dosing (like any other treatment) and patient compliance. Not trying to
(even if it’s with good intentions) force them into what the clinician deems is
best for them.

https://www.rehabps.com/REHABILITATION/Home.html
Words, words, words. Powerful
intangible tools that can create very tangible results, for better or worse. Fear-based
language is common in the clinic, but typically doesn’t get results. And when
it does, then it usually comes with the risk of developing kinesiophobic
behaviors. “Don’t bend forward or your disc will explode”, “Your pain is
because your head is hanging and shearing in front of you”. These are 2
literal quotes I have heard from patients. Whether or not that is what they had
heard from other clinicians (or if that is what they intended) does not matter
as much. Because that is now their perspective on their condition. If the intent is simply to offload painful tissues
or optimize movement we must really reconsider our words for best compliance.
Words matter. There is enough
information out there to show that words really have an impact on a myriad of
areas. Because every word spoken and heard is new information that the central
nervous system (CNS) must process and interpret, then decide what to do with
that information. Take pain sciences for example. There are many clinical leaps
and bounds to give pain science education for everyone with a presentation that
is unfamiliar or complicated. But ever consider to ask and assess if the
patient wants to hear/is ready to hear that information? Postural
corrections are the same. If they aren’t in a state to hear you…telling them
won’t do any good. If they don’t know why it is beneficial for them as individuals
they won’t be present. If you don’t ask for permission to give advice, then you
are often preaching to a wall.
But I get it. Most PT’s are a
bunch of passionate care-bears that can’t help but to help others. It’s in our
blood, it’s why we chose this profession. We are people who want to help
people. We are driven to help the person in front of us so badly that we want
to give them all the possible options even if it means lightly forcing it on
them. Sometimes we care so much that we want to be their only option, the
“fixer” to patient problems. But we have to ease back the “care” sometimes and
reconsider the patients perspective. Perhaps they don’t want the information at
first because they feel that they have not been listened to yet. Perhaps they
don’t want ideal solutions, perhaps they just want to know how they can figure
out how to handle tomorrow. Pain is universal, but the experience is
individual- we cannot assume anything.
However, when it is
appropriate, pain sciences can be amazing and give people hope that what they
are experiencing is normal and can change. It is the same for postural
correctives, when appropriate, it can give the patient relief and empower them
with a bridge to getting better. They see that there is an “escape” for their
pain, even if it is temporary. Perhaps that is all they need to start the chain
of change and they can begin the trust relationship with the clinician.
So how do we change our
words? Sometimes it simply boils down to “stop being the expert” and let the
patient “be their own expert”. Nobody knows them better than themselves. So,
collaborating with the patient can mean empowering the patient with guided
autonomy and tapping into motivational interviewing. Let them sort out the
information you present and co-create a treatment plan. Here’s an example-
If I correct posture and it
decreases their pain, I might follow up with “That’s great! Your pain
decreased! Would you like to wager a guess as to why it changed?”. This gives
an open window to let the patient be inclusive in the reasoning process…this
can either provide an opportunity for a educational blurb if the patient
doesn’t know but is now curious, or you may be surprised and find that
the patient blows your mind with their perspective and reveals something you
would never be able to have known externally. If I were to start with just
telling the patient everything I know, the patient is now being talked at
not talked with.
In regards to maintaining the correctives could be directed via asking, “would you like to know how to maintain (the decrease in pain)?” and then follow up with “could you tell me some strategies to incorporate (the postural correction) into your daily routine?” The patient is now able to give you their best case scenario answers, behavioral strategies, and the most realistic. I most certainly do not know or hope to understand their schedule… however, they can. If they need guiding, we can inquire if they want guidance- “Would you like to hear what has worked for others?”. (I say this all knowing that it can change based on context.)
Seek permission to give information and then empower them to strategize incorporation of treatment.
In regards to maintaining the correctives could be directed via asking, “would you like to know how to maintain (the decrease in pain)?” and then follow up with “could you tell me some strategies to incorporate (the postural correction) into your daily routine?” The patient is now able to give you their best case scenario answers, behavioral strategies, and the most realistic. I most certainly do not know or hope to understand their schedule… however, they can. If they need guiding, we can inquire if they want guidance- “Would you like to hear what has worked for others?”. (I say this all knowing that it can change based on context.)
Seek permission to give information and then empower them to strategize incorporation of treatment.

Jedi Mind Tricks or Motivational Interviewing, call it what you want…But share this post, you will
CONCLUSION:
With clinical reasoning, all
aspects of foundational assessments (particularly posture in this case) become
invaluable lenses for peering into the status of the patient’s CNS and also
into the lives of patients. Postural assessment is a foundational tool that
requires practice and reflection, much like any other foundational tool. I am
still refining this skill by constantly practicing and reflecting, and likely
will forever be doing so. It is definitely not the path of least resistance,
but via deliberate practice of using postural assessments and reflecting on my
clinical reasoning, it has lead me to discover links in their movements
(subtle right?) to many “mystery” pains. The majority of these “mystery pains”
in individuals that are usually concluded to be an unresolvable pain for the
rest of their lives, in my opinion, are simply a consequence of going the path
of least resistance or an inability to embrace the team concept of healthcare.
With medical collaboration, deliberate clinical reasoning, there are so many
patients that could be given hope, hope that allows them to receive effective
treatments and live their lives to the fullest.
Treating a person
holistically, in my opinion, comes from understanding a person intrinsically
and extrinsically. The verbal subjective helps us to understand people
intrinsically, listening not just to what but how the narrative is being said.
Understanding people extrinsically comes from reading into posture because
posture tells their physical story and tells not just a what, but why. We are
simply the translator of both, which, again, requires deliberate practice and
reflection to understand the language.
I’ll end this postural series
with two lessons I’ve learned from two of my PT role models about reflection
and practice.
Joe Donnelly (president of
the Academy of Orthopedic PT, PT and life mentor): His favorite word is
“metacognition”, or “thinking about your thinking”. Optimal clinical reasoning
comes from just that. Going home and struggling with questioning why you did
what you did. So that you face tomorrow with sharper reasoning and further
understanding of “the more you know, the more you realize you don’t know”
spurring continuous learning.
Clare Frank (as you all know, the movement
systems extraordinaire, #Clareified): One of her favorite quotes is from Pablo
Picasso “Learn the rules like a pro, so you can break them like an
artist”. Deliberate practice of the
foundations leads to the creative artistry of being an expert clinician. But
this takes time and effort. So take it slowly and enjoy the beauty of the
method and process. The more you are ‘present’ during your practice, the more
you can see beyond the black and white lines and see the colors beyond. Read
her blogpost on it.
Simply put, posture matters
because all parts of the individual matters. You could just take my word for
it… or take the Movement Links seminar to learn the foundations and then
the DNS courses to learn the beginning of posture and learn for yourself (obviously
the better choice).
Go forth and move well!
(fin)
Blogpost by Josh
Lee, PT, DPT, OCS
Josh is a physical therapist with Mercer University and Piedmont Hospital in Atlanta, GA. He is a board certified orthopedic clinical specialist (Mercer University Ortho Residency graduate), a Movement Links Certified Clinician, current OMPT fellow in training at Mercer University, and primary author of the Postural Considerations chapter in the 3rd edition of the Trigger Point Manual. Josh is an avid movement systems enthusiast and advocate, and aspiring wordsmith.
References:
1. Geist K, Donnelly D. Chapter 66 Soleus and Plantaris Muscles
“Joggers Heel”. In: Donnelly JM, Fernandez-de-las-Penas C, Finnegan M, Freeman
J. Myofascial Pain and Dysfunction The Trigger Point Manual. Philadelphia,
PA: Wolters Kluwer; 2019.
2. Brooker C. Mosby’s 2013 Dictionary of Medicine, Nursing and
Health Professions. 9 ed. Edinburgh, Scotland: Elsevier; 2013.
No comments:
Post a Comment